
The endometrium matters
Much has been discovered in recent decades about eggs, sperm and embryos. About the endometrium, however, little is still known — and some assign it a secondary, almost passive role in reproduction.
We do not see it that way. The endometrium is an active agent in implantation: it can even select the embryo, making it harder for malformed embryos to settle in the uterus. This process is subject to failure — and it is precisely in those failures that studying the endometrium brings answers and helps improve implantation rates.
Endometrial appearance on ultrasound
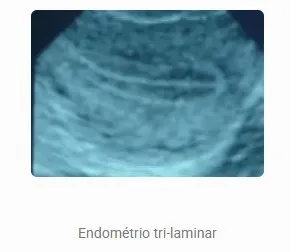
This is the simplest criterion to assess. On ultrasound, the endometrium can have three appearances: linear (during menstruation, generally up to 5 mm); triple or trilaminar (under the effect of female hormones — the pattern desired during stimulation and transfer preparation); and hyperechoic (entirely white, under the effect of progesterone, seen after ovulation or transfer).
As for thickness, the medical literature reports pregnancy from 5 mm, with the best results from 7 mm onward. Values below 5 mm carry an unfavorable prognosis for pregnancy.


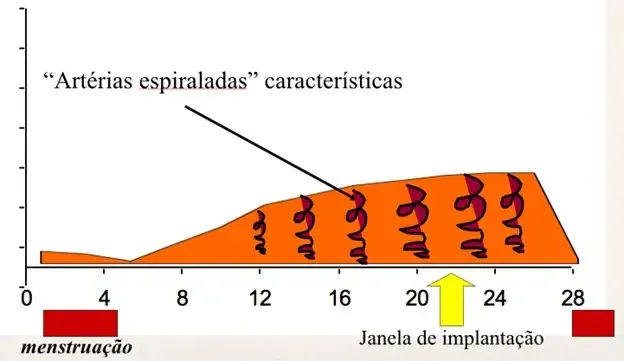
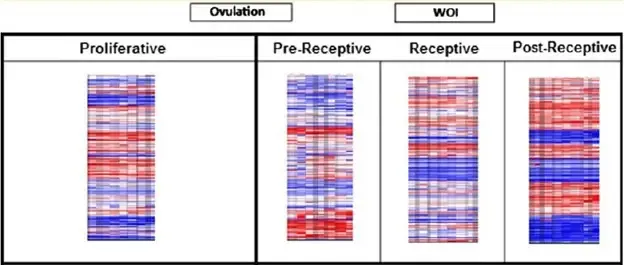
The implantation window
This is the specific period in which implantation can occur — about five days, between the sixth and tenth day after ovulation. The window is defined by ovulation and progesterone production.
If the embryo reaches the uterus before or after the window, it does not implant. The window may also be displaced, too short or too long. A short window helps explain implantation failure even with good-quality embryos; a long window, in which the endometrium loses its ability to select embryos, helps explain recurrent miscarriage.
Implantation markers
From the endometrial sample obtained by biopsy, several markers can be analyzed:
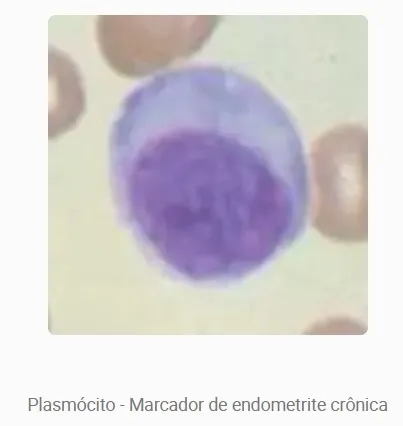
- Plasma cells
- cells linked to antibody production. Their increase indicates endometritis — an infection of the endometrium that, when chronic, causes no symptoms and goes unnoticed, impairing implantation.
- NK cells (CD16 / CD56)
- defense cells that, with altered function, may attack the embryo. An imbalance in the CD16+/CD56+ ratio is associated with lower implantation; there is evidence that human immunoglobulin may help reverse this picture.
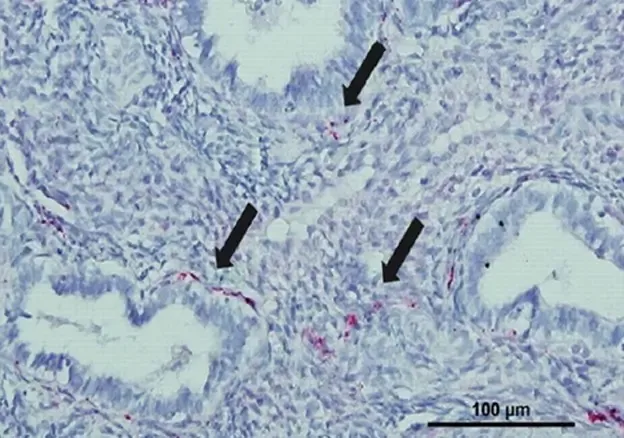
- Nerve fibers (PGP 9.5)
- nerves present in the endometrium of patients with endometriosis — a marker that can avoid a surgery (laparoscopy) performed for diagnosis alone.
- ERA test
- a genetic test that assesses whether the endometrium is receptive. It is rich in scientific information, but currently has little clinical application: faced with a "non-receptive" endometrium there is little to do, and gene manipulation is prohibited by law. For this reason, at Neo Vita we prefer immunohistochemical analysis, which guides concrete decisions.
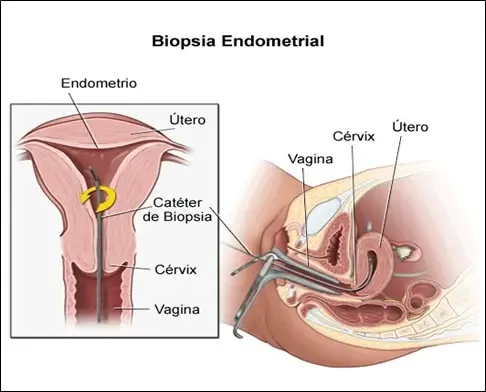
What the endometrial biopsy involves
Also called scratching or endometrial injury, it is a minimally invasive procedure, performed in the office itself, without anesthesia and without an operating room. It is therefore simpler, safer and far less costly than a hysteroscopy.
A thin plastic catheter — the Pipelle de Cornier — is introduced through the cervix into the endometrial cavity and, by suction, collects a small sample. Discomfort is minimal, with slight or no pain and no bleeding. The sample is sent for immunohistochemical analysis, which guides concrete decisions: antibiotics, adjustment of progesterone preparation, human immunoglobulin, anticoagulants.

The biopsy that increases the chances — and the research behind it
The endometrial biopsy has a remarkable additional effect: it increases implantation rates in the following cycles. The likely reason is a change in the endometrium’s immune response pattern, or the formation of a small scar that begins to produce substances that favor implantation.
This effect was first described by the Israeli researcher Barash, in 2003, who observed double the chance of implantation in patients who underwent a biopsy in a cycle prior to in vitro fertilization.
These results were confirmed by us in 2011, in the analysis of the preliminary data from Dr. Fernando Prado’s doctoral thesis on endometrial proteins and embryo implantation. The work was presented at the 27th European Congress of Human Reproduction and Embryology (ESHRE), in Stockholm, and received wide coverage in the national and international press — including British outlets such as the BBC and The Telegraph.

References in the medical literature
- Al-Jefout M, et al. Diagnosis of endometriosis by detection of nerve fibres in an endometrial biopsy: a double blind study. Human Reproduction, 24(12): 3019-24, 2009.
- Salker M, Teklenburg G, Molokhia M, Lavery S, Trew G, et al. Natural Selection of Human Embryos: Impaired Decidualization of Endometrium Disables Embryo-Maternal Interactions and Causes Recurrent Pregnancy Loss. PLoS ONE 5(4): e10287, 2010.
- Barash A, Dekel N, Fieldust S, Segal I, Schechtman E, Granot I. Local injury to the endometrium doubles the incidence of successful pregnancies in patients undergoing in vitro fertilization. Fertility and Sterility 2003; 79:1317-22.
- Bueno MB, Ferreira FP, Maia Filho VOA, Rocha AM, Serafini P, Motta ELA. Local endometrium injury/healing increases embryo implantation and pregnancy rates of in vitro fertilization treatments. Human Reproduction, v. 26, p. i205-i206, 2011.